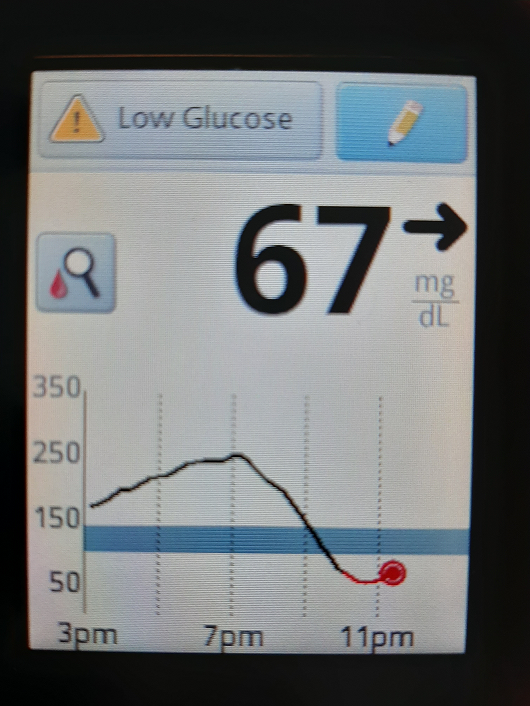
The photo is of my overnight glucose from my Abbott Libre continuous glucose monitor - after an all carb, high carb dinner. I know people who know me are worried that I am now hypoglycemic.
And I see now that what I thought was "50" was closer to one hundred - the bottom of the blue safety line.
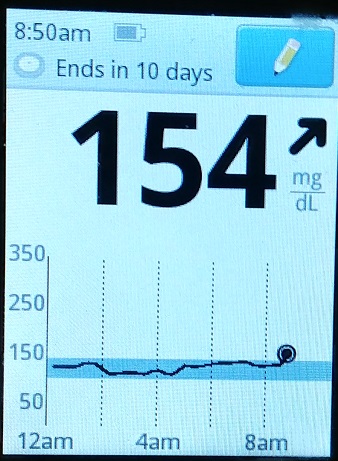
I was telling people that BEFORE I started the new protocol ( almost no fat) the overnight levels were higher, sometimes still in the blue, but often above.
In 3 days following the protocol in Medical Medium, that all changed.
The overnite (liver maintained) glucose levels dropped to the bottom of the blue "safe" line, and sometimes below. Eating ALL carbs. (Until just now, I though it was below 50, probably closer to 90)
For example, last night I went to an Italian restaurant, had a ton of pasta (spaghetti), bread with olive oil (sans the normal butter I would use), large salad, and then home to a lot of desert and a ton of glucose tabs. Yes, I needed insulin, but less, and study the snapshot of my overnight blood sugar with that kind of (High Carb/Low Fat) diet.
The other day we splurged and had two hot dogs - Wham - the overnight steady-state blood sugar was much higher and harder to control.
It is such a different world now. Being able to eat things I like and that taste good to me - so long as no fat, almost any level of carbohydrate feeds the boddy what it needs. I had a rootbeer float for dinner the other night
I, as a profound insulin-dependent diabetic (sans a portion of my pancreas), to be able to eat bread and potatoes and sweets with the only consequence being I have lower blood sugar and less requirement for insulin - so long as I keep total fat to less than 10% of my calories - as Linus Pauling might say, is miraculous.
(And there are some sugars, such as the high fructose corn syrup found in soft drinks, that are not helpful, they are not glucose .)
There is the issue that cancer tumors have 10-times the number of glucose receptors. I will deal with that issue more in the cancer forum, but suffice it to say - if you have an active cancer, you still want to starve it of glucose, because its needs for glucose are even higher than ordinary cells. We know from the Keto experience that you can live being starved for glucose... More in the cancer forum
I am also announcing the first use of a trademark. (September 5, 2019)
World's Finest Glucose (tm)
World's Finest Glucose is a trademark of Immortal Cell Sciences.
This will be a registered trademark, if possible (the wording may be too generic to get it registered) .